————
Part 1: GIDYQ-AA Personal Reflection
Part 2: Psychological Benefits of Diagnostic Confirmation
~ Part 3 in the Gender Dysphoria Diagnosis series ~
Part 4: DSM and ICD Diagnostic Criteria
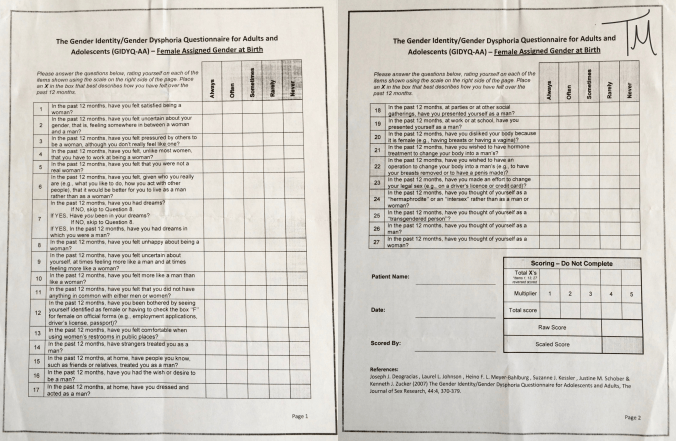
Part 5: GIDYQ-AA Full Text
————

That’s me. A child dressed in baggy boy’s clothes, peeking out from underneath shaggy bangs – hair longer than she wanted but parentally forbidden from getting it cut – playing with her heifer calf named John. A child who knew she was a girl but desperately wanted to be a boy instead.
In a previous post, I discussed my overwhelming doubts about whether or not I truly have gender dysphoria given how atypical my experience seems to be in comparison to the more commonly portrayed trans narratives and the established diagnostic criteria. My experience since puberty has been predominantly characterized by intense physical dysphoria regarding female body characteristics, in the absence of any cognitive gender identity. So I didn’t consider myself “transgender” and I didn’t even know that gender dysphoria (formerly called gender identity disorder) was an established phenomenon or that transition options existed until two years ago – I just thought I had a very unusual and very severe body image disturbance. I have also previously described the powerful relief and peace I felt after having the gender dysphoria diagnosis confirmed by a specialist.
But despite the relief, acceptance, and confidence that followed after receiving expert confirmation of gender dysphoria, I found that after a couple of months those familiar doubts started creeping back in. Contributing to this resurgence of doubt was my ongoing difficulty understanding the significance of my childhood gender experience with respect to my current adult gender experience. Throughout my exploration of the trans community and investigation of transition options over the past two years, I have never been sure to what extent my obvious childhood gender non-conformity (obvious in memory and in family photos) and my distinct childhood desire to be a boy would necessarily add support to an adulthood diagnosis of gender dysphoria. I kept asking myself: how relevant is my childhood gender non-conformity?

That’s me too. A child posing awkwardly in a dress, a child forced into that dress by her rigidly insistent mother, a child hating that dress with a feisty little rage because dresses are impractical and frivolous garments, a girl who wanted to be a boy and resented being forced into a conventional girl’s uniform, but pulling off an admirably convincing smile to please her father holding the camera.
Typical trans narratives on personal blogs and from high-profile trans advocates usually emphasize that they “knew” they were the “opposite” gender since they were extremely young.
“As a child I knew everyone was telling me that I was a boy but I felt like a girl.” – Laverne Cox
“Ever since I could form coherent thoughts, I knew I was a girl trapped inside a boy’s body. There was never any confusion in my mind.” – Jazz Jennings
“For me, I tend to refer to my childhood as one of a transgender child. When I was four and began asserting myself as the girl I knew myself to be… all I knew was that my internal sense of gender, what spoke to my soul, did not align with my body. But my prepubescent body had not grown into this battle I had to fight against.” – Janet Mock
“As far back as four or five I felt like a boy and wished I was a boy.” – Chaz Bono
“My earliest memories were that of wanting to be a girl even before I learned to spell.” – Jade Starr
Most trans people seem to interpret early childhood behaviors and preferences that align with opposite-sex stereotypes as incontrovertible evidence of their gender dysphoria. But research suggests that childhood gender non-conformity is relatively common. “Surveys report that 2-5% of children aged up to seven, as reported by their parents, ‘behaves like opposite sex’ and 1-2% ‘wishes to be of opposite sex.'” (Kaltiala-Heino 2015) And among these gender non-conforming children, only a small minority (ranging from 2-37% in various studies) will retain gender dysphoric feelings into adolescence (Kaltiala-Heino 2015, Smith 2014, Steensma 2013, Wallien 2008). “The evolution of a gender nonconforming child is unpredictable, and it is therefore impossible to determine whether the condition will persist into adolescence or adulthood.” (Meriggiola 2015)
And of course, assessment of whether a child’s behavior is “gender non-conforming” is based on a troubling frame of reference: cultural gender stereotypes and the sexist attitudes associated with deviation from those stereotypes. “Cultural issues likely play a major role in whether a child’s behavior is perceived as gender atypical. Consultations due to gender identity are generally more often sought for boys than girls, which may suggest greater gender variation in boys, but also that effeminate behaviors in boys are perceived as more of a problem than tom-boyishness in girls… that natal boys were more commonly bullied because of gender presentation suggests that effeminate characteristics in boys are less tolerated than masculine self-presentation in girls.” (Kaltiala-Heino 2015)
Research also shows that childhood gender non-conformity is more often associated with adolescent and adult non-heterosexual sexual orientations than with gender dysphoria and transgender identity. “Another issue regarding the psychosexual outcome of children with gender identity disorder is the relation between the child’s gender atypicality and sexual orientation in adulthood. Early prospective follow-up studies indicated that a high rate (60-100%) of children (mostly boys) with gender dysphoria had a homosexual or bisexual sexual orientation in adolescence or adulthood and no longer experienced gender-dysphoric feelings… in accordance with retrospective studies among adult homosexuals, who recalled more childhood cross-gender behavior than heterosexuals. Adult individuals with childhood gender dysphoria are thus much more likely to have a nonheterosexual sexual orientation than a heterosexual sexual orientation.” (Wallien 2008)
In light of that information, I have always been uncomfortable with the strong emphasis that many trans people place on their childhood gender non-conformity. It left me feeling very unsure about how to integrate my own childhood experience into my current perspective regarding a diagnosis of gender dysphoria. And their emphasis also makes me deeply uncomfortable because it perpetuates the idea to the general public (who likely don’t know the statistics regarding low rates of persistence of childhood gender dysphoria into adolescence but who seem to have an exaggerated perception of the association between childhood gender non-conformity and future homosexuality) that childhood cross-sex behavior means their kid is trans or gay. These ideas potentially lead to inappropriate suppression of that behavior by the parents (if parents are homophobic or transphobic and believe they can prevent their kid “becoming” trans or gay). “There is evidence that some clinicians and parents have offered or requested treatment for children with gender identity disorder, in part, to prevent the development of homosexuality.” (Davy 2015) Or these ideas may lead to premature medical or psychological intervention (if parents are supportive of their child’s cross-gender interests but perhaps somewhat misguided and overenthusiastic in pursuing early transition). And clinical experience suggests that it is often the parents’ concern about their child’s gender non-conformity that leads to psychological assessment, rather than the child’s own distress about their gender non-conformity. “Parents of children with gender identity disorder are often ‘unable to cope’ with gender uncertainty… parents most often bring their children to clinical attention… in these cases, it is the parents whose children do not adhere to normative expectations of gender performance who experience ‘distress’.” (Hird 2003) I felt so confused and conflicted about all of this, and I have therefore intentionally avoided discussing my childhood gender experience in any great detail on my blog until now.
Laverne Cox has spoken out about the psychological advantages of puberty suppression in adolescents with gender dysphoria, a procedure which scientific evidence strongly supports as having substantial therapeutic benefit and which allows for more satisfying physical transition outcomes (Smith 2014, Kaltiala-Heino 2015, Meriggiola 2015). But Laverne Cox also promotes transitioning in early childhood, “With transition, the earlier the better. I think if your child knows that they are transgender – and we usually know – then it is life-saving.” I think that is an extremely irresponsible statement for an influential transgender advocate to make, given the existing evidence about the unpredictable psychosexual outcomes in gender non-conforming children.“Medical interventions are not warranted in pre-pubertal children.” (Kaltiala-Heino 2015) Research about the management of gender dysphoria in children recommends a supportive but cautious monitoring approach, with further assessment and consideration of puberty suppression if gender dysphoria does in fact persist past the onset of puberty. “The percentage of transitioned children is increasing and seems to exceed the percentages known from prior literature for the persistence of gender dysphoria, which could result in a larger proportion of children who have to change back to their original gender role, because of desisting gender dysphoria, accompanied with a possible struggle… the clinical management of children with gender dysphoria in general should not be aimed to block gender-variant behaviors.” (Steensma 2013)
To summarize the results of numerous studies: childhood gender dysphoria seems to be associated with an increased likelihood of future homosexual or bisexual orientation, and childhood gender dysphoria may or may not (and usually does not) persist into adolescence. “In clinical practice, gender-dysphoric children and their parents should be made aware of [these outcomes] and, if this would create problems, be adequately counseled.” (Wallien 2008) But of course, childhood “gender non-conformity” may simply represent the beautiful freedom and remarkable creativity inherent in children’s innocent pastimes viewed through an adult lens of social gender stereotypes. Childhood “gender non-conforming” behavior may also be a vital process in the development of their individual identity, not something that requires any parental intervention whatsoever. Let them be kids. Let them figure out for themselves who they are. “It is with seasoned modesty that we emphasize, to different degrees, the changeability of children during growth and development… what children desire of themselves as children is rarely what satisfies them as adults.” (Reiner 2011)
Revisiting the scientific literature on these topics has also had substantial personal relevance, allowing me to reframe my own childhood and adolescent experiences in a way that gives me more confidence in a current diagnosis of gender dysphoria and gives me a deeper understanding of assorted fragments of my increasingly coalescent story.
Knowledge of the factors associated with persistence versus desistance of childhood gender dysphoria into adolescence is limited (Steensma 2013). However, from this limited research, it has been demonstrated repeatedly that one of the most important factors associated with higher rates of persistence of gender dysphoria from childhood into adolescence is the intensity of childhood gender non-conformity or cross-sex identification. “Presentation [of gender dysphoria] is heterogeneous in childhood, with some children exhibiting extreme gender non-conforming behaviors accompanied by severe discomfort and other children showing less intense characteristics. Not all adolescents with gender dysphoria experience symptoms in early childhood, but those who do often present with more extreme gender non-conformity.” (Smith 2014) “Taken together, the prior research suggests that persistence of childhood gender dysphoria is most closely linked to the intensity of the gender dysphoria in childhood and the amount of gender-variant behavior.” (Steensma 2013) My childhood gender non-conformity WAS extremely intense, with a very strong and persistent desire to “be a boy” (in the context of a childish understanding of gender and a naive perception of masculine and feminine stereotypes) and drastic efforts (within a child’s limited scope of control) to create a boyish physical appearance through choice of clothing and hairstyle. The above research lends major relevance to the intensity of my childhood gender dysphoria, rather than the mere presence of it. Which adds diagnostic value to that aspect of my own story, and also allows me to understand the significance of my childhood experience without perpetuating the troublesome misconceptions about childhood gender non-conformity that I described above.
In terms of persistence of childhood gender dysphoria into adolescence, I now understand the significance of my own response to the physical changes accompanying puberty. “Gender dysphoria which intensifies with the onset of puberty usually persists… At puberty, the development of secondary sexual characteristics can lead to increased distress, sometimes leading to severe extremes such as depression, anxiety, self-harm, suicidal tendencies, substance abuse, and high-risk sexual behaviour. Reactions to early pubertal changes have a high diagnostic value.” (Meriggiola 2015) Several other studies also reinforce the “high diagnostic value” of teenagers’ response to development of secondary sexual characteristics in early puberty (Smith 2014, Steensma 2013, Wallien 2008). In contrast to cognitive gender identity (which I suppose I would have described as “wishing to be a boy” when I was a child, but which seemed to fade away at the onset of puberty), my physical dysphoria increased dramatically in response to early pubertal changes. I was so intensely distressed by my budding breasts and broadening hips and my first few periods, that I immediately initiated a regime of strict dietary restriction and excessive exercise to starve away all traces of physical femaleness. These behaviors quickly progressed to full-blown anorexia nervosa, which persisted for the next six years. In retrospect, this experience now has high diagnostic value and is strongly consistent with gender dysphoria.
Not only do reactions to early pubertal changes have “high diagnostic value”, there is also diagnostic value associated with the response to puberty suppression. “Treatment with a GnRH analog [puberty suppression] is thought to be a diagnostic aid as well as a therapeutic intervention for this age group because stopping the progression of the physical changes of puberty would be expected to partially alleviate gender dysphoria symptoms in true gender dysphoria. The first prospective study of psychological outcomes in adolescents… showed a statistically significant improvement in behavior, emotional problems, and general functioning after puberty suppression.” (Smith 2014) I experienced intensified body aversion at the onset of puberty, but through extreme and prolonged starvation I basically created my own puberty suppression protocol (which ideally should have been achieved with appropriate drugs under medical supervision but I wasn’t aware of those options at the time so I did what I could on my own to suppress my confusing physical dysphoria). Anorexia virtually halted further pubertal development: the drastic weight loss induced amenorrhea which lasted from age 13 to 19 and prevented any further increase in chest and hip size, so that I floated through my teenage years in a rail-thin, nearly pre-pubescent, and highly androgynous body. During those years, my eating disorder was its own source of distress (food-related thoughts were incessant and abnormal eating behaviors were pronounced). But that all seemed such a small price to pay to achieve a tenuous and provisional satisfaction and comfort with a less feminine body, a “partial alleviation of gender dysphoria” secondary to “stopping the progression of the physical changes of puberty”. Which aligns precisely with the description in the above study. Once again, this evidence provides very definitive support for a true diagnosis of gender dysphoria in my case.
When I was 19, I experienced my first episode of major depression and I gained nearly 100lbs over a nine-month span. Menstruation resumed, acne worsened, my chest and hips increased in size, and my body basically went through normal puberty after a six-year starvation-induced delay. Following the weight gain and further pubertal development at 19 years old, my body became more feminine and my physical dysphoria escalated to a previously unprecedented intensity, to the point that I could no longer tolerate the sight of myself and began avoiding mirrors and showering in the dark. Moving uncomfortably through the next five years in a much heavier and more feminized body, I would often reflect on my androgynous teenage thinness with an excruciating sense of loss tainting all of those fond memories, a desperate feeling of hopelessness of ever regaining such a genderless and comfortable body. Only in the past year, after having lost some of the weight that I gained six years ago and developing a much more rigorous weightlifting routine to increase my upper body muscle mass, have I been able to create a more satisfying and comfortably androgynous appearance without depending on a dangerously low body weight. So now, when I reflect on my teenage body, those memories are no longer pained by desperation and loss. Instead, those memories have become just one more part of my story that now makes sense. I have finally let go of those last remnants of doubt: I DO have gender dysphoria. Atypical gender dysphoria, sure. But “atypical” tends to be my typical way of life.

That’s me. A skinny teenager sweating in the heat of August summer, her smile genuine this time from the satisfaction of building a rope ladder from sawed-off poplar branches to scale the walls of a hay bale fortress. I can still feel the comforting looseness of those tattered jeans around my narrow hips. I can feel the freedom and lightness and vitality in that slender androgynous body. It is only the slightest rise of my pectoral topography through the kid-sized purple T-shirt that hints at the biological truth I tried to deny.

That’s me. A scrawny kid taking her first solo ride on her brother’s dirtbike, a little wobbly and a little cautious and a lot exhilarated. I can still feel the weight of my brother’s heavy boots on my feet, still feel the wind snatching my breath away as I tossed caution aside and revved up into top speed, still remember how alive I felt in that slim boyish body.

And that’s me too. A lean little nymph leaping so lightly across the scattered hay bales, her favorite green Peter Pan sweater billowing around her weightless self. In the moment before the jump, I felt like I could fly, I felt alive inside my body, and I trusted my body to do what I wanted it to do. So all the muscles in my legs contracted, my feet pushed down hard against the hay, and then, recklessly, I tossed my stick-thin Peter Pan body up… and up… and up… towards a genderless Neverland in the dusky evening sky.
“Lastly, she pictured to herself… how she would keep, through all her riper years, the simple and loving heart of her childhood; and how she would gather about her other little children, and make their eyes bright and eager with many a Wonderland of long ago; and how she would feel with all their simple sorrows, and find a pleasure in all their simple joys, remembering her own child-life, and the happy summer days.”
– Lewis Carroll (Alice’s Adventures in Wonderland, 1865)
————
References
Davy Z. The DSM-5 and the politics of diagnosing transpeople. 2015. Archives of Sexual Behavior 44(5): 1165-76.
Hird MJ. A typical gender identity conference? Some disturbing reports from the therapeutic front lines. 2003. Feminism and Psychology, 13: 181–199.
Kaltiala-Heino R, Sumia M, Työläjärvi M, et al. Two years of gender identity service for minors: overrepresentation of natal girls with severe problems in adolescent development. 2015. Child Adolescent Psychiatry and Mental Health 9: 1-9.
Meriggiola MC, Gava G. Endocrine care of transpeople part I. A review of cross-sex hormonal treatments, outcomes and adverse effects in transmen. 2015. Clinical Endocrinology 83(5): 597-606.
Reiner WG, Townsend Reiner D. Thoughts on the nature of identity: disorders of sex development and gender identity. 2011. Child and Adolescent Psychiatric Clinics of North America 20(4): 627-38.
Smith KP, Madison CM, Milne NM. Gonadal suppressive and cross-sex hormone therapy for gender dysphoria in adolescents and adults. 2014. Pharmacotherapy 34(12): 1282-97.
Steensma TD, McGuire JK, Kreukels BP, et al. Factors associated with desistence and persistence of childhood gender dysphoria: a quantitative follow-up study. 2013. Journal of the American Academy of Child and Adolescent Psychiatry 52(6): 582-90.
Wallien MS, Cohen-Kettenis PT. Psychosexual outcome of gender-dysphoric children. 2008. Journal of the American Academy of Child and Adolescent Psychiatry 47(12): 1413-23.