————
Part 1: GIDYQ-AA Personal Reflection
~ Part 2 in the Gender Dysphoria Diagnosis series ~
Part 3: Childhood Gender Non-Conformity
Part 4: DSM and ICD Diagnostic Criteria
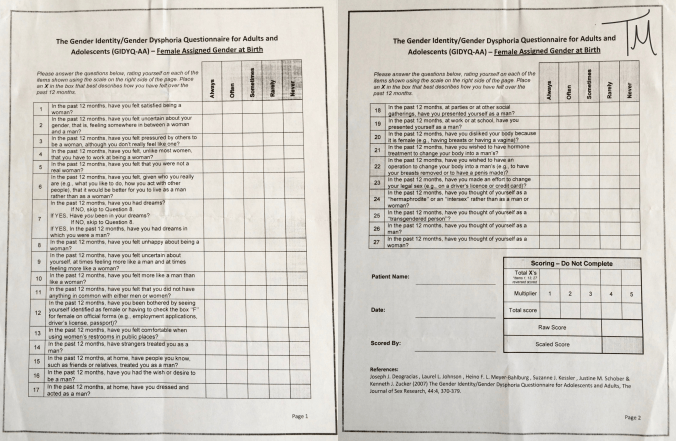
Part 5: GIDYQ-AA Full Text
————

In a previous post, I described the intense relief and peacefulness that I felt after receiving confirmation of a diagnosis of gender dysphoria from an experienced psychiatrist. Confirmation of the diagnosis helped reduce the overwhelming doubt and uncertainty (what’s wrong with me? do I really have gender dysphoria? or is this something else?) and helped me move towards acceptance. Acceptance of gender dysphoria facilitated the freedom to start considering transition options without being constantly tugged backwards by relentless nagging doubt regarding the diagnosis itself.
From my personal experience, it seems that most trans people have a strong intrinsic sense of their own gender identity and most trans people feel much more confident than I did in aligning themselves with the established criteria for gender dysphoria and in pursuing transition. My psychiatrist, who specializes in working with transgender people, told me that most of his patients are confident regarding their transition goals and just need help accessing resources to transition when they initially present to his clinic. One study described a group of adolescents referred for assessment at a gender clinic in Finland: “During the assessment process, 72% (34/47) of the applicants were sure about feeling they were of the opposite sex to their natal and about pursuing sex reassignment, but 28% (13/47) were not sure about their feelings regarding gender identity and/or sex reassignment.” (Kaltiala-Heino 2015) Those results support my anecdotal impressions that the majority of trans people feel certain about their gender identity and transition goals.
But even for trans people who are more certain of their gender identity and transition goals than I was, the potential psychological benefit derived from diagnostic confirmation of gender dysphoria should not be underestimated.
A prospective study published in 2014 evaluated the psychological response to different steps in gender reassignment therapy in people with gender identity disorder (GID) (the old term for what is now called gender dysphoria). “To our knowledge, it is the first publication that focuses on the effects of the separate parts of the sex reassignment therapy.” (Heylens 2014)
The study recruited participants from a population of patients who applied for sex reassignment therapy at a Gender Clinic in Belgium. These patients had not previously received a diagnosis of GID and had not initiated any medical aspects of transition (such as hormone therapy or surgery) prior to applying to the Gender Clinic. A total of 82 patients agreed to participate in the study after giving informed consent, however 12 were excluded from the study because they did not meet the criteria for GID (they were instead given the diagnosis of GID-NOS, gender identity disorder not otherwise specified), another 12 patients were excluded from the study because they did not undergo “full treatment (hormonal and surgical)” due to psychiatric/medical comorbidities (3 patients) or personal preferences regarding transition goals (9 patients), and 1 patient was excluded from the study because they committed suicide during follow up. This left 57 patients in the study (46 MTFs and 11 FTMs) diagnosed with GID who completed all steps (hormonal and surgical) in the gender reassignment process.
Supporting the results of many previously published articles, this study showed that, “Sex reassignment therapy does influence the level of psychopathology in GID patients, with significant reduction in anxiety, depression, somatization, psychoticism, interpersonal sensitivity, hostility, and overall psychoneurotic distress… after treatment, the majority of patients indicated that they have a better mood, are happier, and feel less anxious than before. They also seem to be more self-confident and encounter a better body-related experience, indicating a less distorted self-image than before treatment.” (Heylens 2014)
Of particular relevance here, the results from this study showed that out of all the steps involved in gender reassignment therapy, confirmation of the GID diagnosis and initiation of hormone treatment were associated with the greatest psychological benefit. “The most important effect seemed to result from the confirmation of the diagnosis and the initiation of hormone therapy.” (Heylens 2014) The results strongly suggest that diagnostic confirmation of GID is, in itself, a very important and affirming step for patients.
However, based on the participant exclusion criteria, I think the results of this study may actually underestimate the positive psychological effects of diagnostic confirmation. The study excluded patients who did not strictly meet the GID criteria (an excluded group which may have included some non-binary trans people with less definitive cross-sex identity) and excluded patients who did not complete all steps of the gender reassignment process (the majority of whom chose not to based on personal preferences regarding transition). This suggests that the final population of patients in this study (those who received a formal diagnosis of GID and went on to complete all the steps in transitioning to the opposite sex) may have had a relatively high degree of certainty regarding their gender identity and transition goals compared to a broader population of patients (such as those with a GID-NOS diagnosis or patients who desired some but not all aspects of transition). The authors partially acknowledge this bias when they discuss the limitations of their study: “On the whole, our study population is a selected group that is not fully representative for the larger group of gender dysphoric people: they all fulfilled criteria for GID and were eligible for SRS. This perspective might certainly have an influence on the level of psychoneurotic distress. If there had been less certainty, at the end of the diagnostic phase and after initiation of hormonal treatment, about receiving SRS, results could have been different.”
Yet even in this population of gender dysphoric patients with potentially greater confidence and certainty regarding transgender identity and transition goals compared to a more diverse group, it is clear that the confirmation of the diagnosis (GID) by a professional was one of the most important steps in the transition process with respect to psychological improvements. “We found that the biggest decrease in psychological dysfunctioning is caused by initiation of hormone therapy or confirmation of the diagnosis by a professional caregiver. This finding was consistent with the subjective feeling of most treated patients and suggests that recognition and acceptance of the GID play an important role in the transition process.”
Recognition and acceptance. Isn’t that what we all want?
“If you’ll believe in me, I’ll believe in you.”
– The Unicorn (Through the Looking-Glass and What Alice Found There, 1871)
————
References
Heylens G, Verroken C, De Cock S, et al. Effects of different steps in gender reassignment therapy on psychopathology: a prospective study of persons with a gender identity disorder. 2014. Journal of Sexual Medicine 11(1): 119-126.
Kaltiala-Heino R, Sumia M, Työläjärvi M, et al. Two years of gender identity service for minors: overrepresentation of natal girls with severe problems in adolescent development. 2015. Child Adolescent Psychiatry and Mental Health 9: 1-9.