
“I’m interested in contemporary vision – the flicker of chrome, reflections, rapid association, quick flashes of it. I don’t do anecdotes; I accumulate experiences.”
– James Rosenquist (interview for Creative Loafing, 2003)
“I’m interested in contemporary vision – the flicker of chrome, reflections, rapid association, quick flashes of it. I don’t do anecdotes; I accumulate experiences.”
– James Rosenquist (interview for Creative Loafing, 2003)

“The system should treat all user input as sacred.”
– Jef Raskin (The Humane Interface: New Directions for Designing Interactive Systems, 2000)

Materials: ballpoint pen (black) + black fine-point Sharpie marker + Staedtler colored pencils
Time: 20 hours
Reference: photo of myself taken August 14, 2016. I look tired, because it was taken very early in the morning. And I look sad, because I’d said an indefinite goodbye to someone I love two days before. I took this photo because I realized that I’d never drawn sadness.
Comments: it was very difficult for me to complete this sketch. My style has improved a lot since I first started drawing portraits, but increased skill creates higher expectations, and I was disappointed to feel my old paralyzing perfectionism emerging once more. And drawing my own sadness meant that I was reminded – over and over – of the reasons for that sadness. Fighting perfectionism and embracing sadness for the duration of this drawing was emotionally exhausting. But I found that I was more comfortable drawing a self portrait this time. After my first self portrait, I said I liked my eyes and my hair and my collarbone. After my second self portrait, I realized – with great surprise! – that I actually like my whole face.

“She was a genius of sadness, immersing herself in it, separating its numerous strands, appreciating its subtle nuances. She was a prism through which sadness could be divided into its infinite spectrum.”
– Jonathan Safran Foer (Everything is Illuminated, 2003)
————
Part 1: Drugs and Doses
~ Part 2 in the Testosterone series ~
————
After a long process of clarifying my transition goals, I was finally able to create a prescription plan to help achieve a more androgynous appearance without complete masculinization. I initially felt confident about my plans for hormone therapy. However, in the weeks leading up to my appointment with a new family doctor who could provide these prescriptions, I began to feel more uncertain about starting testosterone – I wondered whether recent improvements in body image could be sustained without drugs, and I was concerned about potential side effects even on low doses of T and finasteride.
I also felt anxious that the doctor may not understand or support my atypical transition goals. In my experience, people’s ignorance of gender dysphoria can often lead to misunderstanding or hostility and judgment. But people’s knowledge of gender dysphoria, from personal or professional experience, can also create frustrating barriers to understanding and acceptance. Other trans people, whose experience aligns more closely with typical trans narratives, often respond defensively or dismissively to my uncertainty about gender identity and my ambivalence about pursuing medical transition options. Medical professionals, whose work with other trans patients informs their perspective on gender dysphoria, often convey wildly inaccurate assumptions about my experience. These assumptions usually become evident in their well-intentioned attempts to demonstrate knowledge and acceptance. But these assumptions do not make me feel accepted; they make me feel invisible.
When I arrived for my appointment, it was immediately apparent that the doctor had made some problematic assumptions. He assumed that I wanted to achieve maximum masculinization as quickly as possible – before I had even mentioned my transition goals, he delivered several warnings about the risks of taking too much testosterone and several reassurances that I should start seeing physical changes very soon on standard doses. He assumed that he would have to educate me about hormone therapy – he interrupted me constantly to deliver very basic information that I already knew. And he assumed that I would trust his opinion – he emphasized the fact that he had worked with “lots” of trans patients to support his recommendations, with little reference to specific clinical experiences or published literature.
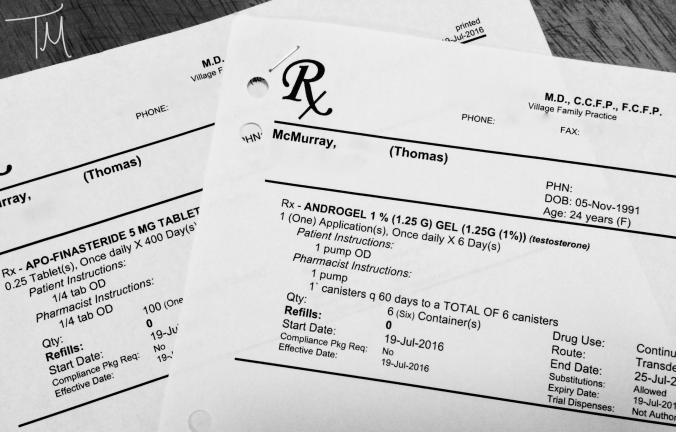
His inaccurate assumptions and his tendency to interrupt meant that it took much longer than necessary for me to explain my situation. Eventually, in an abbreviated and fragmented fashion, I was able to describe my transition goals. He said that my experience is “atypical” and admitted that he doesn’t have many patients who want to transition slowly and partially. But by the end of the appointment, he seemed to understand my perspective and he was supportive of my desire to proceed cautiously (or potentially not even start T right away). He gave me the prescriptions I requested: 1.25g/day Androgel and 1.25mg/day finasteride.
I mentioned my concern about T potentially causing mood fluctuations (less likely with lower doses and transdermal formulations). He cheerfully reassured me that mood issues aren’t a problem in patients on much higher doses of injectable T, so he would expect no changes in mood on the dose of Androgel that I requested, although I might experience slightly increased energy on T. While that information was somewhat comforting, I wondered if there may be some bias in his clinical experience which could lead to underestimation of the effects of T on mood. I have previously described how trans people may tailor the information they share with doctors who control access to transition options. If someone is desperate to continue hormones but experiences negative mood side effects, they might be motivated to withhold that information from the doctor to avoid being told to decrease the dose or discontinue hormones.
I also mentioned my fear that T could cause increased appetite and significant weight gain. Even if the weight gain was related to a desirable increase in muscle mass, these sides effects would be very difficult for me to cope with due to a long history of disordered eating. He again cheerfully reassured me that weight gain is usually minimal even on higher doses of T, typically characterized by a slight increase in muscle mass with concurrent decrease in body fat so that the number on the scale may remain stable or increase by only a few pounds. He said that people who do experience significant weight gain after starting T are generally gaining weight for reasons other than the hormones, so if I maintained the same exercise and diet routine after staring T then I shouldn’t expect much change in weight and appetite. Changes in body weight can be assessed more objectively than changes in mood, so it seems that clinicians’ observations of weight changes are less likely to be biased by selective disclosure from patients.
Finally, I asked him whether long-term use of low-dose T would eventually lead to complete masculinization (just on a much slower timeline than higher doses) or whether it would allow partial masculinization to a stable endpoint that could be sustained and non-progressive over time. The doctor was very confident in saying that it would be the latter (partial non-progressive masculinization). But I have found no published evidence to support either conclusion, and the doctor admitted that he has “very few” patients who elect to start on a low dose of T (let alone maintain a low dose of T indefinitely) so it seems that his clinical experience with respect to this question would be relatively limited. [Several weeks later, I discussed the same question with a psychiatrist who specializes in working with transgender people. The psychiatrist said that the endocrinologists he’s worked with believe long-term low-dose T would eventually (over decades) lead to complete masculinization, which directly contradicts the family doctor’s response to my question. It seems there are no definitive answers available].
So I left the appointment with two prescriptions and more questions than answers. My instinctive desire for certainty grappled with my relentless tendency for skepticism. I was grateful that I had been given the prescriptions I requested, grateful that I had the freedom to move forward with hormone therapy whenever I wanted – a freedom that many trans people do not have. But as I reviewed the prescriptions and the lengthy consent form outlining all potential risks and side effects, I still found myself questioning more intensely whether this drugs are truly right for me, or whether I could find a way to be comfortable in this XX body without hormonal or surgical intervention.
“We make all sorts of assumptions because we don’t have the courage to ask questions.”
– Miguel Ruiz (The Four Agreements: A Practical Guide to Personal Freedom, 2001)
