I have spent much of the past two years researching gender dysphoria and exploring what it means to be transgender. This process has often been frustrating and confusing, as I have had considerable difficulty reconciling my intense physical dysphoria related to the female aspects of my body with the absence of any internal sense of “gender identity”. But after this prolonged immersion in the online trans community, in-depth review of the scientific literature on trans issues, and personal experience with transgender support groups and mental health professionals, the most prominent source of my chronic confusion has become apparent.
The “gender identity” concept, typical transgender narratives, and the criteria for diagnosis of gender dysphoria all depend on gender stereotypes – stereotypes which are increasingly irrelevant in modern society and which research overwhelmingly suggests are cultural constructs with limited biological underpinning. “One of the first steps to liberating people from the cage that is gender is to challenge established gender norms.” (Reilly-Cooper 2016) I think the dependance of “gender identity” discourse, trans narratives, and gender dysphoria diagnostic criteria on these gender norms actually serves to reinforce outdated and restrictive stereotypes rather than dismantle or challenge those stereotypes.
Much of this post will directly quote statements made by other authors in scientific review papers or online articles (bold indicates my own added emphasis). My goal here is not to simply repeat what has already been so eloquently stated elsewhere. I refer readers to the sources referenced at the bottom of this post for more thorough discussion of various related issues.
Instead, I wish to organize these statements within a coherent framework. This framework demonstrates a troubling and self-reinforcing cycle: the concept of “gender identity” relies on problematic gender stereotypes, the typical trans narrative relies on “gender identity” as an explanation and justification for choices regarding transition, and the diagnostic criteria for gender dysphoria use conventional gender norms as the frame of reference for assessment and diagnosis. In a clinical context, trans people are thus motivated to present their experiences in a way that aligns with opposite-gender norms to facilitate diagnosis of gender dysphoria and gain access transition options. But aligning themselves with cross-gender stereotypes necessarily (and paradoxically) requires acknowledgment of the restrictive and oppressive nature of those stereotypes which are associated so strongly (but unjustifiably) with biological sex. To counter this contradiction, trans people then invoke the concept of a discrete and inborn “gender identity” to assert the legitimacy of their experience.
(Note: This is a lengthy post with dense content. However, my conclusions are carefully derived from in-depth analysis of the concepts and research outlined throughout this post, so I encourage readers to work their way through my arguments slowly and sequentially to fully understand my final conclusions).
(1) “Gender Identity” Concept
“Gender identity is a highly problematic concept.” (Hird 2003)
Typical trans narratives strongly emphasize behaviors and preferences that align with cross-gender stereotypes as evidence of an intrinsic “gender identity”, based on a faulty assumption that there are inherent qualitative differences between men and women to support the existence of those stereotypes in the first place. The conceptualization of “gender identity” as an innate internal property is the “crucial tension at the heart of gender identity politics”. (Reilly-Cooper 2016)
“In this research, ‘gender identity’ is characterized as a sense of oneself as male, female, or indeterminate, whereas ‘gender role’ is characterized as behaviors, personality traits, and interests that society applies to these aspects, and the way that people are measured against stereotypical attributes.” (Davy 2015) But is it really possible to separate “gender identity” from those “stereotypical attributes” that constitute “gender role”? To what extent do those “stereotypical attributes”, and the values and judgments that society assigns to those attributes, contribute to the development of “gender identity”?
I think “gender identity” is best understood as a constructed cognitive self-perception arising from internalized cultural gender stereotypes. “Gender variance may be conceptualized, as gender variant people apparently already do, as a multidimensional or sometimes idiosyncratically conceptualized, multicategorical construct.” (Cohen-Kettenis 2009) “It is clear from feminist research that behaviors are not intrinsically masculine or feminine, but change through time and in different spaces… Gender constructionist research suggests that biological imperatives are few in the human, and consist only of procreative imperatives. Other behavioral aspects such as sartorial preference, aggression, empathy, and intelligence, among a number of other characteristics, are not sex specific and are often adaptable… recent research situates behavioral sex differences firmly within a social role model… This unresolved debate weakens any possibility of arguing that there is something inherent in masculine and feminine behaviors. (Trans) people have never been subjects of an independent masculine or feminine type, and combinations of what is deemed masculine or feminine at any one time can be found within all humans, albeit performed with different intensities.” (Davy 2015)
Indeed, research regarding the development of identity during childhood consistently describes “gender identity” as an aspect of self-perception that develops and evolves over time in response to many internal and external factors. Factors contributing to the construction of gender identity include genetics, hormones, socialization, and progressive cognitive understanding of gender. (Hines 2011, Reiner 2011) “Gender development is multidimensional, and developmental processes involved in each dimension are likely to differ.” (Hines 2011) Gender identity is an “evolving sense of self as one sex or the other.” (Reiner 2011) Evidence suggesting that “gender identity” develops and changes over time in response to many different factors directly contradicts the commonly held belief that “gender identity” is an innate and immutable property. The low rate of persistence of childhood gender dysphoria into adolescence also contradicts the idea that “gender identity” is an inborn and unchanging entity.
“Gender identity is woven pervasively throughout identity.” (Reiner 2011) It is also clear that “gender identity” is simply one of many facets of identity which develop over time. Therefore, “gender identity” cannot be regarded as something discrete and separate from overall identity, and “gender identity” cannot be regarded as immune to the internal and external factors contributing to the ongoing development of overall identity.
“The precise mechanisms of gender identity development are complex, the interactions of the mechanisms poorly understood, and the outcomes not entirely clear, except that children and adolescents nearly always dichotomize.” (Reiner 2011) This tendency to dichotomize “gender identity” reflects persistent societal adherence to opposing gender stereotypes. Gendered socialization and the influence of this socialization on cognitive understanding of gender are major factors contributing to the development of “gender identity”. “Socialization factors also gain in importance, as parents and then peers and eventually teachers encourage children to engage in gender-typed play. The child also begins to develop the understanding that he or she is male or female, and this knowledge produces motivation to imitate the behavior of others of the same sex.” (Hines 2011) As described above, this gendered socialization occurs despite the overwhelming evidence demonstrating that gender stereotypes have limited biological underpinning and that behaviors, preferences, personality traits, and cognitive functioning are not sex-specific attributes. (Hines 2011, Davy 2015) It is well established that societal gender stereotypes vary widely across different cultures and across different historical time periods (Hird 2003). This argues against any innate human “gender identity” giving rise to subsequent behaviors and preferences stereotypically associated with biological sex. Rather, it supports the idea that socially constructed gender norms give rise to individual “gender identity”.
I think the biggest weakness of the “gender identity” concept is that it is promoted as being real, immutable, and innate (endogenous) yet it remains so vague and poorly defined by those who claim to experience it. “The [trans] advocates’ websites rarely offer any indication of what feeling like a man or a woman is like.” (Davy 2015) Attempts to describe what “feeling like a man” or “feeling like a woman” means invariably fall back on conventional societal (exogenous) masculine or feminine stereotypes. This creates a frustratingly circular logic: “gender identity” is a property that is supposedly experienced internally (and therefore cannot be denied by an external perspective) but which cannot be defined in any way separate from externally imposed gender norms.
This has been extremely perplexing for me. This is why I have tried very hard to describe my experience of gender dysphoria in a concrete and clearly defined way that does not depend on reference to an internal “gender identity”. My previous blog posts (here, here, and here) have recounted the distressing thoughts and emotions that arise in response to seeing or touching the female secondary sexual characteristics of my body. This is the only way I can explain my experience without resorting to dichotomous gender stereotypes.
I do not know WHY my female anatomy generates such intense distress for me. I only know that it DOES. It would certainly be convenient to say that my physical dysphoria is secondary to a mismatch between my anatomy and my “gender identity”. But I fail to understand the concept of “gender identity” and I refuse to align my personal preferences and behaviors and interests with problematic and oppressive gender stereotypes for the sake of convenience. My female body (and the irrational but undeniable distress arising from my perception of it) and my human personality (my preferences, behaviors, and interests) are two separate things. “Gender is the value system that ties desirable (and sometimes undesirable?) behaviours and characteristics to reproductive function. Once we’ve decoupled those behaviours and characteristics from reproductive function – which we should – and once we’ve rejected the idea that there are just two types of personality and that one is superior to the other – which we should – what can it possibly mean to continue to call this stuff ‘gender’? What meaning does the word ‘gender’ have here, that the word ‘personality’ cannot capture?” (Reilly-Cooper 2016)
Some might argue that my claiming an absence of “gender identity” merely represents an “agender” or “non-binary” identity along a “gender spectrum”. But those terms are simply variations on the original “gender identity” concept, and therefore remain inapplicable. Rebecca Reilly-Cooper presents an excellent series of arguments explaining why the conceptualization of gender as a spectrum is not really any more progressive or inclusive than a gender binary with two opposite poles. Rather, the concept of gender as a spectrum is illogical. I encourage readers to review her essay in full but will summarize her conclusions here: “If gender identity is a spectrum, then we are all non-binary, because none of us inhabits the points represented by the ends of that spectrum… Once we recognize that the number of gender identities is potentially infinite, we are forced to concede that nobody is deep down cisgender, because nobody is assigned the correct gender… at birth. In fact, none of us was assigned a gender… at birth at all. We were placed into one of two sex classes on the basis of our potential reproductive function, determined by our external genitals. We were then raised in accordance with the socially prescribed gender norms for people of that sex. We are all educated and inculcated into one of two roles, long before we are able to express our beliefs about our innate gender identity, or to determine for ourselves the precise point at which we fall on the gender continuum. So defining transgender people as those who at birth were not assigned the correct place on the gender spectrum has the implication that every single one of us is transgender; there are no cisgender people. The logical conclusion of all this is: if gender is a spectrum, not a binary, then everyone is trans. Or alternatively, there are no trans people. Either way, this a profoundly unsatisfactory conclusion, and one that serves both to obscure the reality of female oppression, as well as to erase and invalidate the experiences of transsexual people. The way to avoid this conclusion is to realize that gender is not a spectrum. It’s not a spectrum, because it’s not an innate, internal essence or property. Gender is not a fact about persons that we must take as fixed and essential, and then build our social institutions around that fact. Gender is socially constructed all the way through, an externally imposed hierarchy, with two classes, occupying two value positions: male over female, man over woman, masculinity over femininity.” (Reilly-Cooper 2016)
(2) Typical Transgender Narratives
As a highly pathologized, stigmatized, and marginalized community, trans people are placed in a very difficult position with respect to how they describe their experience. In a clinical context, trans people must present their narrative in a way that meets the established diagnostic criteria for gender dysphoria (criteria which are based on “cross-gender identification” and evidence of behaviors and preferences stereotypically associated with the “other sex”) in order to gain access to transition therapies. In a public context, trans people must present their stories in a way that is understandable to society at large, in order to promote awareness and acceptance. Because gender stereotypes are so deeply woven into the fabric of our society, describing trans experiences in terms of strong preferences for opposite-sex stereotypes arising from an innate “gender identity” allows a publicly palatable and understandable (albeit oversimplified and problematic) narrative to emerge from within an already well-established gender framework.
“Research has suggested that adult transpeople often think that if they do not express stereotypical masculinities and femininities… they will not fit the model that may steer them to the transitioning healthcare pathways… many transpeople are reluctant to relay anything to gender clinic psychiatrists that might be viewed as different from the perceived “correct” trans narrative. In previous research, I have demonstrated that transpeople tend to tailor their clinical narratives because they realize that psychiatrists have the power to stop their transitioning process… transpeople retrospectively claim to have participated in stereotypically gendered play and behaviors when they have sought transitioning technologies, and have often interspersed expected gender inflections into their clinical narratives… These inflections seem inevitable because the diagnostic criteria expect cross-gendered play and behaviors to be performed prior to the granting of transitioning technologies… the clinically expected expressions of gender do not correspond well to gender role play or leisure pursuits apparent in contemporary society.” (Davy 2015)
The typical or “correct” trans narrative seems to include these main elements: strong retrospective emphasis on the early onset of gender dysphoric feelings in childhood which persisted into adolescence and adulthood, gender dysphoric feelings arising primarily from discomfort with societal gender stereotypes, assertion of a supposedly intrinsic and fixed “gender identity”, and physical dysphoria portrayed as a secondary consequence of a primary mismatch between the brain’s “gender identity” and the body’s “assigned sex”. To put it more simply, the typical trans narrative says: from a young age my personality and preferences did not align with conventional binary gender roles and gender stereotypes, therefore I must have a cross-gender or non-binary “gender identity”, therefore I must be transgender, therefore I am trapped in the wrong body, therefore my body needs to be changed to align with my “gender identity”. “Transpeople have often defined their trans gender identities through a ‘‘wrong body’’ narrative.” (Davy 2015)
Typical trans narratives not only emphasize the concept of an innate “gender identity”, they also imply that this cross-sex “gender identity” is the result of pre-natal biological factors. “Trans advocates’ essentialist claims of gender dysphoria seem to assume that society will be more accepting of transpeople if they are understood to have been ‘‘born this way”… [due to] the relative power that biogenetic discourses maintain in society and particularly in medicine.” (Davy 2015) The etiology of gender dysphoria is not clearly understood, but one of the most common theories is that exposure to altered levels of sex hormones during fetal development leads to “sex-atypical cerebral programming that diverges from the sexual differentiation of the rest of the body”. (Hoekzema 2015) However, “no evidence thus far has linked normal variability in the early hormone environment to gender dysphoria.” (Hines 2011) Additionally, people with disorders of sexual development (intersex conditions) that do cause abnormal exposure to sex hormones in utero overwhelmingly maintain a “gender identity” that aligns with the sex they were assigned at birth, rather than with the sex that their pre-natal hormone exposure more closely mimics (Hines 2011, Reiner 2011). “The majority of intersex people identified their gender as their sex assigned at birth.” (Reiner 2011) For example, female fetuses (XX chromosomes) with congenital adrenal hyperplasia have a genetic defect in adrenal enzyme pathways that leads to accumulation of androgens (such as testosterone) in the fetus’ body and causes pre-natal virilization of the female genitals. These infants are assigned female at birth. Despite high levels of pre-natal androgen exposure and masculinized genitalia, 97% of women with CAH identity as female from childhood into adulthood (Hines 2011). Male fetuses (XY chromosomes) with androgen insensitivity syndrome have normal testes and normal androgen production but lack androgen receptor molecules, which means that testosterone produced by the testes has no effect on the developing fetus. Androgen insensitivity impairs the masculinization of male genitalia in the developing fetus and the development of male secondary sexual characteristics during puberty. These XY individuals are often raised as females (particularly in cases of complete androgen insensitivity) and maintain a female “gender identity” despite having a male chromosomal configuration. (Reiner 2011) These examples provides strong evidence that “gender identity” is influenced more strongly by socialization and external gender expectations than internal biological factors like sex hormone exposure or sex chromosomes.
The typical trans narrative centers around a supposedly innate “gender identity” as an explanation for their discomfort in the body and the social role associated with their biological sex and as justification for their choices regarding transition. But as I outlined above, the concept of “gender identity” as a fixed internal property has no logical or scientific basis and relies entirely on an external frame of reference (societal gender stereotypes). “Trans advocates’ essentialist claims of gender dysphoria… and the desire to transition to a particular gender tend to mirror the simplistic dualisms from biological research, in which masculinity and femininity are regarded as natural, rather than socially constructed, characteristics.” (Davy 2015) So the emphasis on, and continued perpetuation of, the “gender identity” concept by trans advocates only serves to reinforce outdated and oppressive stereotypes.
(3) Gender Dysphoria Diagnostic Criteria
“Gender dysphoria is not always a straightforward diagnosis. This can be ascribed to the fact that international classifications are quite general and have significant short-comings, there are no objective criteria, and gender dysphoria can present in a great diversity of forms, situations, and experiences.” (Fabris 2015)
Most of the medical and psychological research regarding gender dysphoria has been based on diagnostic criteria in the American Diagnostic and Statistical Manual of Mental Disorders (DSM). I have focused on articles published since 2000, which usually refer to the diagnostic criteria for gender identity disorders in the DSM-IV and DSM-IV-TR (published in 1994 and 2000, respectively) or the criteria for gender dysphoria in the DSM-5 (published in 2013). However, some recent studies still refer to the criteria for gender identity disorders in the WHO International Statistical Classification of Diseases, the ICD-10 (published in 1993).
With respect to the DSM criteria, there is a glaring lack of validity studies or evidence supporting inter-rater reliability in the diagnostic process (Cohen-Kettenis 2009). It has been suggested that validity of the DSM diagnostic criteria can be inferred from studies evaluating sex reassignment as a treatment procedure. “Sex reassignments based on DSM diagnoses primarily resulted in satisfying results, in terms of alleviating the discomfort about one’s sex or the ‘gender dysphoria.’ Although diagnosis and response to sex reassignment are not very closely connected, and the reported findings are certainly no ‘‘proof’’ of the correctness of the diagnosis, they suggest that the elements of the DSM diagnosis are clinically useful.” (Cohen-Kettenis 2009) However, in the studies referenced by that statement, most of the subjects underwent “complete” sex reassignment. So the inferred clinical utility of DSM criteria may only apply to those who desire all aspects of sex reassignment, which is not representative of the transition goals of all trans people. “Indeed, clinicians in gender identity clinics are increasingly confronted with treatment goals other than complete sex reassignment.” (Cohen-Kettenis 2009) So the utility of the existing diagnostic criteria is, at best, limited to a subpopulation of the diverse transgender community.
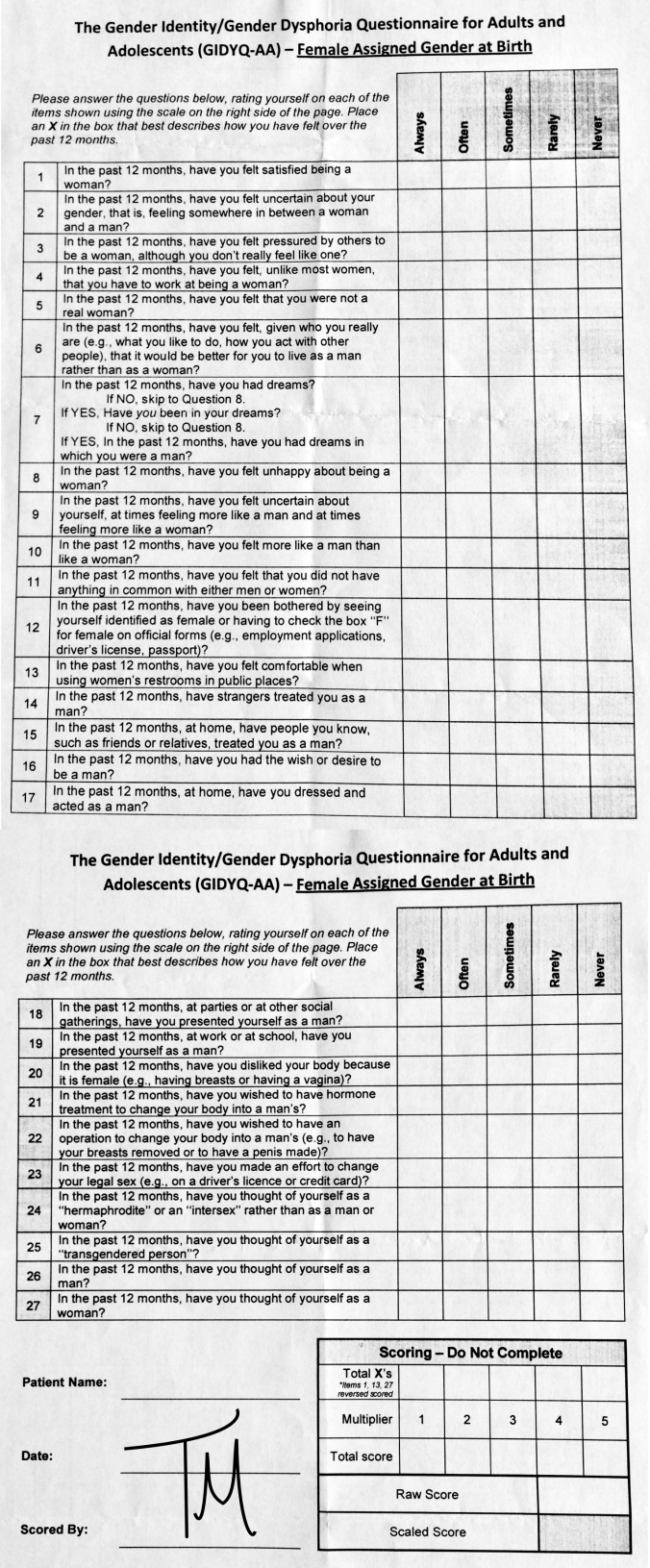
One of the primary criticisms regarding the diagnostic criteria for gender identity disorder in the DSM-IV and DSM-IV-TR was the inability of the criteria to reflect the diversity of gender variance. “A problem with the current criteria is that gender identity, gender role, and gender problems are conceptualized dichotomously rather than dimensionally. For instance, the DSM-IV text states that adults with gender identity disorder are preoccupied with their wish to live as a member of the other sex, manifested as an intense desire to adopt the role of the other sex or to acquire the physical appearance of the other sex through hormonal or surgical manipulation. Within the gender identity disorder criteria, a concept such as ‘‘cross-gender identification’’ also assumes that there are only two gender identity categories, male and female.” (Cohen-Kettenis 2009) I have previously discussed my frustration that even supposedly dimensional (rather than dichotomous) scales used to measure the intensity of gender dysphoria (such as the GIDYQ-AA) leave little room for non-binary responses, and interpretation of the questions on the survey relies heavily on the reader’s alignment with stereotypical roles behaviors associated with men and women.
Prior to publishing the updated version of the DSM (DSM-5) in 2013, a workgroup was developed to revise the gender identity disorder criteria. One of the biggest revisions was a change in diagnostic terminology from gender identity disorder to gender dysphoria, to emphasize the distress associated with gender variance as being a form of psychopathology rather than gender non-conformity being considered pathological in and of itself. The goal of the workgroup was to revise the criteria in a way that would help destigmatize trans people while maintaining a diagnostic category that medical insurance companies would accept to provide financial support for transition treatments. (Davy 2015)
However, despite those revisions, the current DSM-5 criteria for gender dysphoria remain problematic. “The diagnostic framework in the DSM-5 for all transpeople continues to be underpinned by essentialist, heteronormative assumptions that situate binary sexes – male and female – with corresponding genitalia as the anchor from which gender dysphoria is judged… I would argue that the criteria proposed by the DSM-5 are derived from stereotypes applied in the gender identity clinics serving transpeople, rather than empirically developed from biological imperatives.” (Davy 2015)
Particularly disturbing is the fact that the research and clinical experience taken into account in revising the DSM-5 diagnostic criteria was based heavily on trans peoples’ clinical narratives, which (as I described above) are often tailored with added gender inflections to align more closely with the previously established criteria in order to gain access to transition options. “The DSM-5 Workgroup has disregarded the plethora of work in feminist social science which criticizes the inherency of gender roles, gender identities, and sex differences, as well as research in transgender studies that depicts non-dysphoric transpeople, desires for different embodiments, non-conventional transitioning trajectories, and sexualities. In the pre-publication reports, the Workgroup considered only the views and evidence derived from sexological research. As such, the review reflects a form of expert clinical consensus based on transpeople’s tailored narratives and questionable ideas around masculinity and femininity.” (Davy 2015)
Such a narrow-minded approach to developing diagnostic criteria based on increasingly irrelevant and biologically unjustified gender stereotypes creates a self-perpetuating cycle: trans people present their experiences in ways that align with the criteria, and the criteria are then perceived as being reinforced and validated by their alignment with trans people’s narratives. “The criteria used to diagnose gender dysphoria help psychiatrists to determine whether someone is experiencing distress about incongruence with their experienced gender through a gender normative frame… Arguably, this leads to the situation where transpeople must express incongruent behavior and demonstrate to the psychiatrist that they have most often preferred activities that are traditionally gendered and opposite to those gender norms applied to their assigned sex at birth. Within the DSM-5, these traditional gendered expressions seem to be required in spite of the lack of stark behavioral differences between the genders in Western societies today.” (Davy 2015)
And the ongoing emphasis on “gender identity” as part of the typical trans narrative and as a core diagnostic criterion further reinforces restrictive societal stereotypes. “[Most gender clinic psychiatrists] adhere to gender identity as both ‘‘real’’ and fixed. This adherence then facilitates the continued use of highly stereotyped notions of gender to provide the framework for assessing and treating transsex individuals.” (Hird 2003)
Neither the diagnostic framework nor the professionals involved in the diagnostic process seem to recognize these problems. “Most of the clinicians seemed to take the view that individual solutions are to be sought rather than societal change – there was little suggestion that society requires any change… the clinician’s job is not to reinforce gender boundaries defined by society.” (Hird 2003)
(4) Transition as Self-Determination
I have outlined the major issues regarding the concept of “gender identity”, typical transgender narratives, and the criteria for diagnosis of gender dysphoria. I have expressed my concern that the continued dependence of “gender identity”, trans narratives, and diagnostic criteria on traditional gender norms serves to reinforce restrictive and damaging stereotypes.
My conclusion is that an inborn, immutable, intrinsic “gender identity” DOES NOT EXIST. “Gender identity” is a cognitive aspect of self-perception constructed from internalized societal gender stereotypes. The idea of an innate “gender identity” is a crutch that trans people are forced to use to legitimize their experience in the face of a society that revolves around these oppressive gender stereotypes and a psychiatric establishment that retains these troublesome stereotypes as the frame of reference for assessment and access to transition options.
A self-determination and human rights model of trans identities views the “diagnostic use of stereotypical gendered expressions associated with boys/men and girls/women as erroneous, and that they have little to do with actual contemporary gender identity formations. Accordingly, any gendered expressions, regardless of which birth-assigned sex one is given, should not act as criteria for diagnosing transpeople.” (Davy 2015)
For those who argue that inclusion of gender variance under the umbrella of psychiatry is necessary to allow access to medical and legal transition options, I would point out that some countries have already set a precedent where this is not the case. “Psychiatric involvement in healthcare pathways and legal assistance for those people who want to have a different body and/or corrected legal gender assignment should not be a requirement. They have succeeded in securing this in France, Denmark, Argentina, and Malta. In these countries, transpeople are legally recognized and are given access to healthcare services despite psychiatry being removed as the gatekeeper, because of transpeople demanding healthcare and legal recognition through a self-determination model of gender variance.” (Davy 2015)
“The solution is not to reify gender by insisting on ever more gender categories that define the complexity of human personality in rigid and essentialist ways. The solution is to abolish gender altogether. We do not need gender. We would be better off without it. Gender as a hierarchy with two positions operates to naturalize and perpetuate the subordination of female people to male people, and constrains the development of individuals of both sexes… You do not need to have a deep, internal, essential experience of gender to be free to dress how you like, behave how you like, work how you like, love who you like… The solution to an oppressive system that puts people into pink and blue boxes is not to create more and more boxes that are any colour but blue or pink. The solution is to tear down the boxes altogether.” (Reilly-Cooper 2016)
“Gender identity” needs to disappear. “Transition” should be removed from a gender context and the term “transgender” should be rendered obsolete. Instead, the medical, legal, and social aspects involved in “transition” should be viewed – simply and respectfully – as a human right to self-determination. “Assuming an inner-self who desires such a transformation, gender transitions are thus situated in a non-essentialized experiential framework, anchored in self-determination.” (Davy 2015) People – ALL people, not just trans people – should be free to modify their physical attributes, adopt social roles, and pursue interests that align with their personal preferences and desires. We are all of us “transitioning” all the time, as we learn and grow and adapt to an ever-changing world. “Transition” (in a transgender context) is just one of many ways that people strive for self-expression that makes them feel comfortable. “Transition” (in a human context) is an ongoing process for each of us to create an authentic self in this vast ocean of human diversity.
“If there’s no meaning in it, that saves a world of trouble, you know, as we needn’t try to find any.”
– The King (Alice’s Adventures in Wonderland, 1865)
————
References
Cohen-Kettenis PT, Pfafflin F. The DSM diagnostic criteria for gender identity disorder in adolescents and adults. 2010. Archives of Sexual Behavior 39(2): 499-513.
Davy Z. The DSM-5 and the politics of diagnosing transpeople. 2015. Archives of Sexual Behavior 44(5): 1165-76.
Fabris B, Bernardi S, Trombetta C. Cross-sex hormone therapy for gender dysphoria. 2015. Journal of Endocrinological Investigation 38(3): 269-82.
Hines M. Gender development and the human brain. 2011. Annual Review of Neuroscience 34: 69-88.
Hird MJ. A typical gender identity conference? Some disturbing reports from the therapeutic front lines. 2003. Feminism and Psychology, 13: 181–199.
Hoekzema E, Schagen SE, Kreukels BPC, et al. Regional volumes and spatial volumetric distribution of gray matter in the gender dysphoric brain. 2015. Psychoneuroendocrinology 55: 59-71.
Reilly-Cooper R. Gender is not a spectrum. 2016. Aeon. Accessed online 2016-07-10. (Quotes in this post were extracted from the Aeon article. However, a similar essay also appears on the author’s personal blog More Radical With Age: “Gender is not a binary, it’s a spectrum: some problems”, January 2016).
Reiner WG, Townsend Reiner D. Thoughts on the nature of identity: disorders of sex development and gender identity. 2011. Child and Adolescent Psychiatric Clinics of North America 20(4): 627-38.