
“I’m interested in contemporary vision – the flicker of chrome, reflections, rapid association, quick flashes of it. I don’t do anecdotes; I accumulate experiences.”
– James Rosenquist (interview for Creative Loafing, 2003)
“I’m interested in contemporary vision – the flicker of chrome, reflections, rapid association, quick flashes of it. I don’t do anecdotes; I accumulate experiences.”
– James Rosenquist (interview for Creative Loafing, 2003)

“The system should treat all user input as sacred.”
– Jef Raskin (The Humane Interface: New Directions for Designing Interactive Systems, 2000)

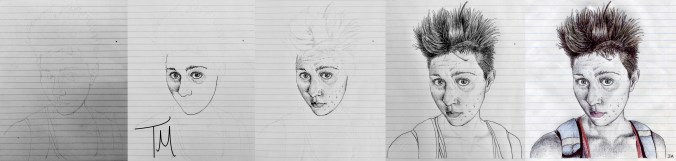
Materials: ballpoint pen (black) + black fine-point Sharpie marker + Staedtler colored pencils
Time: 20 hours
Reference: photo of myself taken August 14, 2016. I look tired, because it was taken very early in the morning. And I look sad, because I’d said an indefinite goodbye to someone I love two days before. I took this photo because I realized that I’d never drawn sadness.
Comments: it was very difficult for me to complete this sketch. My style has improved a lot since I first started drawing portraits, but increased skill creates higher expectations, and I was disappointed to feel my old paralyzing perfectionism emerging once more. And drawing my own sadness meant that I was reminded – over and over – of the reasons for that sadness. Fighting perfectionism and embracing sadness for the duration of this drawing was emotionally exhausting. But I found that I was more comfortable drawing a self portrait this time. After my first self portrait, I said I liked my eyes and my hair and my collarbone. After my second self portrait, I realized – with great surprise! – that I actually like my whole face.

“She was a genius of sadness, immersing herself in it, separating its numerous strands, appreciating its subtle nuances. She was a prism through which sadness could be divided into its infinite spectrum.”
– Jonathan Safran Foer (Everything is Illuminated, 2003)

“Things can harden meaningfully in the moment of indecision.”
– John Ashbery (Self-Portrait in a Convex Mirror, 1975)

And then a Plank in Reason, broke,
And I dropped down, and down –
And hit a World, at every plunge,
And Finished knowing – then –– Emily Dickinson
(I felt a Funeral, in my Brain, 1896)

————
~ Part 1 in the Testosterone Series ~
Part 2: Assumptions and Questions
————
When I initially reviewed the literature on hormone therapy for FTMs over a year ago, I hoped to find quick and easy answers about testosterone. At that time, I had a simplistic and optimistic belief that gender dysphoria was the main issue contributing to depression and other life issues, so I felt a desperate urgency to start medical transition as soon as possible. But because I was still so unsure about my own transition goals, my research felt disorganized and overwhelming and served only to magnify the intensity of my uncertainty.
But after resolving my chronic confusion with the concept of “gender identity,” deconstructing many of my own illusions about my appearance, creating a more concrete mental image of my “ideal” body, and gaining a greater measure of acceptance of my current body, I was finally able to consider hormone therapy with more clarity. As I described previously, my “ideal” body does not align with that of typical cisgender men. Rather, my “ideal” body would have somewhat more masculine facial features and a slightly more masculine silhouette than my current female frame (broader shoulders, more upper body muscle mass, wider waist, narrower hips), but would otherwise be more androgynous than masculine. So I revisited my old research with this new lens, and I was able to create what seemed to be an optimal hormone therapy plan to accomplish my desired physical changes.
It is beyond the scope of this post to summarize all of the published information regarding hormone therapy for FTMs. I present here my own tentative prescription plan with reference to information most relevant to my situation. I hope this may be valuable to others seeking to achieve slight and gradual physical masculinization outside standard FTM hormone therapy protocols. Recent publications have acknowledged increasing diversity in transition goals among gender dysphoric individuals. (Fabris 2006)
————
Testosterone (T): 1-2g/day transdermal
Transdermal T is available as a gel or as a patch. I planned to consult with my prescribing physician about the availability and cost of those options in my area. Injectable (intramuscular) T formulations are most commonly preferred and prescribed for FTMs. (Simpson 2006, Meriggiola 2015) However, compared to the various injectable T formulations, transdermal T has several advantages with respect to my own transition goals.
First, transdermal formulations are associated with more stable serum T concentrations over time that mimic the physiologic secretion of T in cisgender men. (Simpson 2006, Meriggiola 2015) Intramuscular injections of T every 1-4 weeks cause supraphysiologic serum concentrations in the first few days after the injection, followed by a rapid decrease in T concentration. (Meriggiola 2015) Some studies report changes in energy and more pronounced mood swings associated with these rapid fluctuations in T concentration. (Simpson 2006, Meriggiola 2015) Mood changes include more frequent irritability, frustration/anger, and aggression as well as decreased positive and negative affect intensity. (Slabbekorn 2001, Simpson 2006) Maintaining a more consistent T concentration may help reduce mood changes, which is an important consideration for me given repeated episodes of severe depression.
Second, transdermal T may be associated with more gradual physical changes compared to injectable T. (Simpson 2006) “Transdermal formulations are recommended if slower progress is desired or for ongoing maintenance after desired virilization has been accomplished.” (TransHealth UCSF 2016). However, at comparable doses, transdermal and injectable T are associated with a similar overall degree of physical masculinization despite the slower progression of changes occurring with transdermal preparations. (Merrigiola 2015) Many FTMs hope to achieve pronounced physical masculinization as quickly as possible, but given my more conservative transition goals, I would prefer more gradual changes so that I have a longer period of time to evaluate whether the physical changes are truly desirable.
Third, transdermal T eliminates the requirement of giving myself intramuscular injections. I have an embarrassingly low pain tolerance, so I will admit that the prospect of injecting several millilitres of viscous oil into myself every few weeks is very unappealing.
Disadvantages of transdermal T in my situation include increased cost (my current health coverage is limited and does not include the off-label prescription of T for gender transition) as well as possibility for delayed cessation of menstruation (menstruation has always been a core source of body dysphoria for me and is one of the primary motivations to seek hormone therapy). (Simpson 2006) However, other studies have found that transdermal T induces amenorrhea on a similar timeline as injectable T. (Pelusi 2014)
The recommended maintenance dose range of transdermal T for FTMs who want to achieve considerable masculinization as quickly as possible is 2.5-10g per day. (Simpson 2006, Fabris 2015, Meriggiola 2015) A dose of 1-2g per day would likely allow even more gradual progress. Lower starting doses, such as 2.5g per day, are also recommended if there are concurrent psychiatric problems.(Simpson 2006)
Finasteride: 1mg/day oral
I previously discussed my desire to avoid hair loss by using finasteride concurrently with T. In addition to reducing male-pattern baldness in FTMs, finasteride can also be associated with slowed or decreased facial and body hair growth and slowed or decreased clitoromegaly. (TransHealth UCSF 2016) These effects are usually listed as disadvantages in articles about hormone therapy in FTMs. However, given my desire for only slight physical masculinization, these side effects are actually advantages because they align closely with my transition goals. The recommended dose of oral finasteride is 1mg/day. (Mella 2010)
————
In the process of more seriously considering hormone therapy and trying to develop my own prescription plan, I returned to an important question from a previous post:
In an XX person, would long-term administration of low dose T ultimately lead to complete physical masculinization, but at a much slower pace than higher doses of T? Or would long-term administration of low dose T lead to partial masculinization that would be sustainable and non-progressive past a certain point? I am hoping very strongly for the latter. I have started looked for published data to answer this question, but so far I have only found articles describing the effects of long-term administration of high dose T in FTMs or describing the effects of short-term administration of low dose T in women (including the effects of exogenous T administered to treat various medical conditions as well as the effects of endogenous T in women with polycystic ovarian syndrome). However, there seem to be no studies describing the effects of long-term administration of low dose T in female-bodied people without concurrent medical issues.
I want to achieve a sustainable, non-progressive, partial physical masculinization. But I am not sure to what extent this goal is possible, even with conservative use of low dose hormones.
The scientific literature regarding long-term outcomes of low dose T administration in healthy XX individuals is almost non-existent. The literature regarding the extent and timeline of physical and psychological changes on low dose T is also extremely limited. Virtually everything currently published in scientific journals about T-induced changes in FTMs describes study participants on doses of T that are 2-10 times higher than the doses I’m considering. (Fabris 2015, Meriggiola 2015, Slabbekorn 2001, Pelusi 2014) There are some anecdotal reports of the effects of low dose T on blogs and YouTube videos by transmasculine people, but their comments tend to be sporadic, unstructured, and inconsistent.
This scarcity of published information about the short-term and long-term effects of low dose T contributes to my chronic difficulty imagining a future version of myself. For those of us with atypical transition goals, most of the existing medical knowledge and established hormone protocols are simply not applicable. This creates a painful sense of isolation and confusion, as though I’m peering out at the rest of the world from behind a foggy looking-glass.
“It’s dreadfully confusing!”
– Alice (Lewis Carroll, Through the Looking-Glass and What Alice Found There, 1871)
————
References
Fabris B, Bernardi S, Trombetta C. Cross‐sex hormone therapy for gender dysphoria. 2015. Journal of Endocrinological Investigation 38(3): 269-282. Note: see Table 3 for an extensive summary chart regarding testosterone doses and formulations.
Mella JM, Perret MC, Manicotti M, et al. Efficacy and safety of finasteride therapy for androgenetic alopecia: a systematic review. 2010. Archives of Dermatology 146(10):1141-1150.
Meriggiola MC, Gava G. Endocrine care of transpeople part I: a review of cross-sex hormonal treatments, outcomes and adverse effects in transmen. 2015. Clinical Endocrinology 83(5):597-606.
Pelusi C, Costantino A, Martelli V, et al. Effects of three different testosterone formulations in female-to-male transsexual persons. 2014. Journal of Sexual Medicine 11(12): 3002-3011.
Simpson AJ, Goldberg J. Trans Care: Hormones – A Guide for FTMs. 2006. Trans Care Project.Vancouver, BC, Canada. Accessed through Rainbow Health Ontario. Note: see page 5 for a brief summary chart regarding testosterone doses and formulations.
Slabbekorn D, van Goozen SHM, Gooren LJG, et al. Effects of cross-sex hormone treatment on emotionality in transsexuals. 2001. International Journal of Transgenderism 5(3):2.
TransHealth UCSF. Primary care protocol for transgender patient care: hormone administration. Accessed online 26-04-2016.

“Two things you should know about me. The first is that I am deeply suspicious of people in general. It is my nature to expect the worst of them. And the second is that I am unexpectedly good with computers.”
– Veronica Roth (Divergent, 2011)
————
Part 1: GIDYQ-AA Personal Reflection
Part 2: Psychological Benefits of Diagnostic Confirmation
Part 3: Childhood Gender Non-Conformity
Part 4: DSM and ICD Diagnostic Criteria
~ Part 5 in the Gender Dysphoria Diagnosis series ~
————
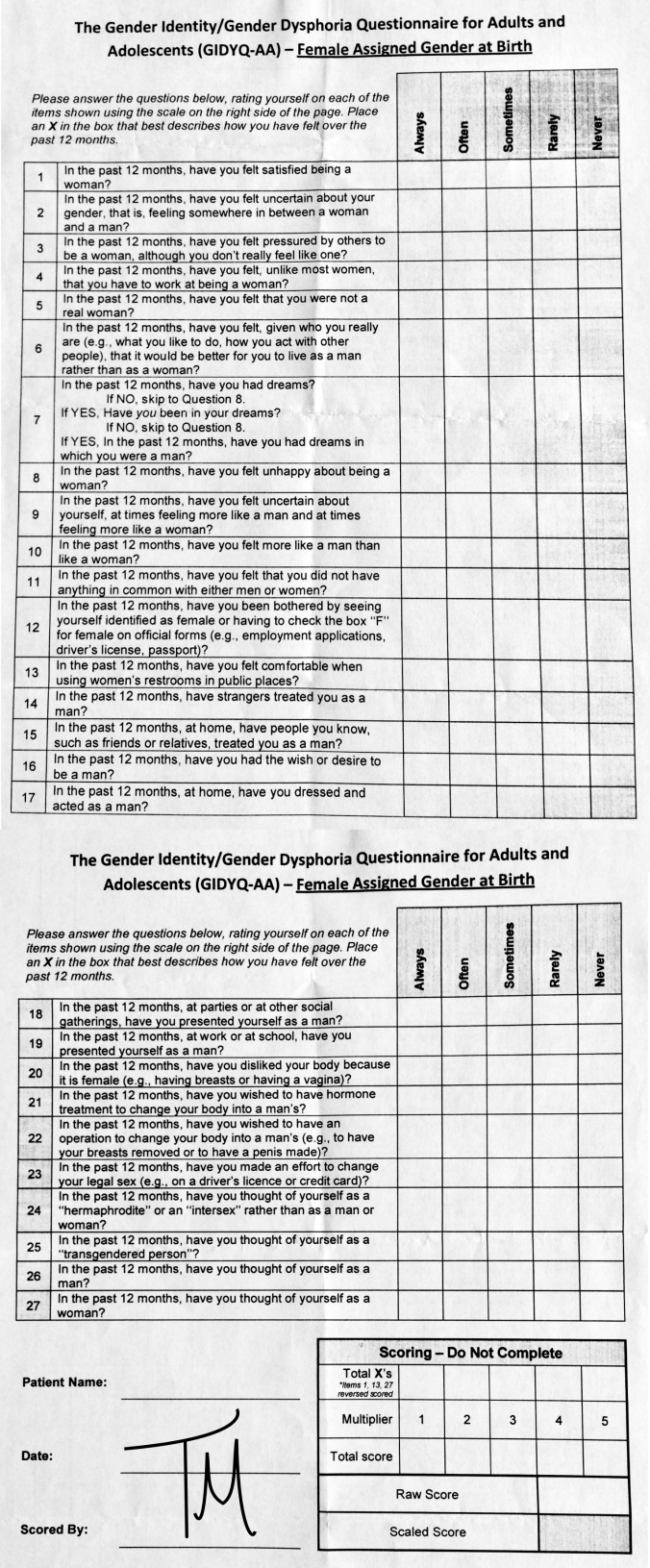
The most commonly viewed post on this blog is Part 1 of this series: GIDYQ-AA Personal Reflection. The popularity of this post likely reflects considerable curiosity regarding the diagnostic process for gender dysphoria. Part 1 only listed a handful of questions from the questionnaire in the context of my personal reflection. It is nearly impossible to find a complete version of the GIDYQ-AA online without access to scientific journals through academic servers, so I thought it might be helpful for readers to dedicate a post to the full text of the GIDYQ-AA.
Below, I have recorded the Female Assigned at Birth and Male Assigned at Birth versions of the GIDYQ-AA in their entirety. I created my own GIDYQ-AA documents formatted for printing, including a table to record responses to questions and a section for scoring; these documents are available for download. I also have a section describing the scoring process in detail. Finally, abstracts from the study describing initial development of the GIDYA-AA (Deogracias 2007) and from a study providing further evidence to support the validity of the GIDYQ-AA (Singh 2010) are also included.
————
GIDYQ-AA Documents for Download
Female Assigned at Birth (Adult) Word
Female Assigned at Birth (Adult) PDF
Female Assigned at Birth (Adolescent) Word
Female Assigned at Birth (Adolescent) PDF
Male Assigned at Birth (Adult) Word
Male Assigned at Birth (Adult) PDF
Male Assigned at Birth (Adolescent) Word
Male Assigned at Birth (Adolescent) PDF
————
GIDYQ-AA (Female Assigned at Birth) Full Text
Response options are “always,” “often,” “sometimes,” “rarely,” or “never.” Items 1, 13, and 27 were reversed scored. For adolescents < 18 years of age, the word woman was changed to girl. Items 1-2, 5-10, 16, and 24-27 were considered to be subjective indicators of gender identity/gender dysphoria. Items 3-4, 11, 13-15, and 17-19 were considered social indicators. Items 20-22 were considered somatic indicators. Items 12 and 23 were considered sociolegal indicators.
01. In the past 12 months, have you felt satisfied being a woman?
02. In the past 12 months, have you felt uncertain about your gender, that is, feeling somewhere in between a woman and a man?
03. In the past 12 months, have you felt pressured by others to be a woman, although you don’t really feel like one?
04. In the past 12 months, have you felt, unlike most women, that you have to work at being a woman?
05. In the past 12 months, have you felt that you were not a real woman?
6. In the past 12 months, have you felt, given who you really are (e.g., what you like to do, how you act with other people), that it would be better for you to live as a man rather than as a woman?
07. In the past 12 months, have you had dreams? If NO, skip to Question 8.
If YES, Have you been in your dreams?
If NO, skip to Question 8. If YES, In the past 12 months, have you had dreams in which you were a man?
08. In the past 12 months, have you felt unhappy about being a woman?
09. In the past 12 months, have you felt uncertain about yourself, at times feeling more like a man and at times feeling more like a woman?
10. In the past 12 months, have you felt more like a man than like a woman?
11. In the past 12 months, have you felt that you did not have anything in common with either men or women?
12. In the past 12 months, have you been bothered by seeing yourself identified as female or having to check the box “F” for female on official forms (e.g., employment applications, driver’s license, passport)?
13. In the past 12 months, have you felt comfortable when using women’s restrooms in public places?
14. In the past 12 months, have strangers treated you as a man?
15. In the past 12 months, at home, have people you know, such as friends or relatives, treated you as a man?
16. In the past 12 months, have you had the wish or desire to be a man?
17. In the past 12 months, at home, have you dressed and acted as a man?
18. In the past 12 months, at parties or at other social gatherings, have you presented yourself as a man?
19. In the past 12 months, at work or at school, have you presented yourself as a man?
20. In the past 12 months, have you disliked your body because it is female (e.g., having breasts or having a vagina)?
21. In the past 12 months, have you wished to have hormone treatment to change your body into a man’s?
22. In the past 12 months, have you wished to have an operation to change your body into a man’s (e.g., to have your breasts removed or to have a penis made)?
23. In the past 12 months, have you made an effort to change your legal sex (e.g., on a driver’s licence or credit card)?
24. In the past 12 months, have you thought of yourself as a “hermaphrodite” or an “intersex” rather than as a man or woman?
25. In the past 12 months, have you thought of yourself as a “transgendered person”?
26. In the past 12 months, have you thought of yourself as a man?
27. In the past 12 months, have you thought of yourself as a woman?
————
GIDYQ-AA (Male Assigned at Birth) Full Text
Response options are “always,” “often,” “sometimes,” “rarely,” or “never.” Items 1, 13, and 27 were reversed scored. For adolescents < 18 years of age, the word man was changed to boy. Items 1-2, 5-10, 16, and 24-27 were considered to be subjective indicators of gender identity/gender dysphoria. Items 3-4, 11, 13-15, and 17-19 were considered social indicators. Items 20-22 were considered somatic indicators. Items 12 and 23 were considered sociolegal indicators.
01. In the past 12 months, have you felt satisfied being a man?
02. In the past 12 months, have you felt uncertain about your gender, that is, feeling somewhere in between a man and a woman?
03. In the past 12 months, have you felt pressured by others to be a man, although you don’t really feel like one?
04. In the past 12 months, have you felt, unlike most men, that you have to work at being a man?
05. In the past 12 months, have you felt that you were not a real man?
06. In the past 12 months, have you felt, given who you really are (e.g., what you like to do, how you act with other people), that it would be better for you to live as a woman rather than as a man?
07. In the past 12 months, have you had dreams? If NO, skip to Question 8.
If YES, Have you been in your dreams?
If NO, skip to Question 8.
If YES, In the past 12 months, have you had dreams in which you were a woman?
08. In the past 12 months, have you felt unhappy about being a man?
09. In the past 12 months, have you felt uncertain about yourself, at times feeling more like a woman and at times feeling more like a man?
10. In the past 12 months, have you felt more like a woman than like a man?
11. In the past 12 months, have you felt that you did not have anything in common with either women or men?
12. In the past 12 months, have you been bothered by seeing yourself identified as male or having to check the box “M” for male on official forms (e.g., employment applications, driver’s license, passport)?
13. In the past 12 months, have you felt comfortable when using men’s restrooms in public places?
14. In the past 12 months, have strangers treated you as a woman?
15. In the past 12 months, at home, have people you know, such as friends or relatives, treated you as a woman?
16. In the past 12 months, have you had the wish or desire to be a woman?
17. In the past 12 months, at home, have you dressed and acted as a woman?
18. In the past 12 months, at parties or at other social gatherings, have you presented yourself as a woman?
19. In the past 12 months, at work or at school, have you presented yourself as a woman?
20. In the past 12 months, have you disliked your body because it is male (e.g., having a penis or having hair on your chest, arms, and legs)?
21. In the past 12 months, have you wished to have hormone treatment to change your body into a woman’s?
22. In the past 12 months, have you wished to have an operation to change your body into a woman’s (e.g., to have your penis removed or to have a vagina made)?
23. In the past 12 months, have you made an effort to change your legal sex (e.g., on a driver’s licence or credit card)?
24. In the past 12 months, have you thought of yourself as a “hermaphrodite” or an “intersex” rather than as a man or woman?
25. In the past 12 months, have you thought of yourself as a “transgendered person”?
26. In the past 12 months, have you thought of yourself as a woman
27. In the past 12 months, have you thought of yourself as a man?
————
————
GIDYQ-AA Scoring
The table at the bottom of the photo above shows how the questionnaire is scored. The scoring process is the same for the female-assigned-at-birth and the male-assigned-at-birth versions. I have summarized the scoring process in more detail below.
Based on published studies evaluating the GIDYQ-AA, a Scaled Score less than 3.0 is strongly suggestive of gender dysphoria, while a Scaled Score greater than 3.0 is more likely to reflect the absence of gender dysphoria. However, no single questionnaire or scoring system can perfectly capture all of the variation in gender identity and personal goals (and I have previously discussed many of the problems that I think may interfere with the utility of the questionnaire), so scores on the GIDYQ-AA are not necessarily definitive and should not replace each individual’s sense of their own identity.
————
“The present study reports on the construction of a dimensional measure of gender identity (gender dysphoria) for adolescents and adults. The 27-item gender identity/gender dysphoria questionnaire for adolescents and adults (GIDYQ-AA) was administered to 389 university students (heterosexual and nonheterosexual) and 73 clinic-referred patients with gender identity disorder. Principal axis factor analysis indicated that a one-factor solution, account ing for 61.3% of the total variance, best fits the data. Factor loadings were all >.30 (median, .82; range, .34-96). A mean total score (Cronbach’s alpha, .97) was computed, which showed strong evidence for discriminant validity in that the gender identity patients had significantly more gender dysphoria than both the heterosexual and nonheterosexual university students. Using a cut-point of 3.00, we found the sensitivity was 90.4% for the gender identity patients and specificity was 99.7% for the controls. The utility of the GIDYQ-AA is discussed.” (abstract, Deogracias 2007)
“This study aimed to provide further validity evidence for the dimensional measurement of gender identity and gender dysphoria in both adolescents and adults. Adolescents and adults with gender identity disorder (GID) were compared to clinical control (CC) adolescents and adults on the Gender Identity=Gender Dysphoria Questionnaire for Adolescents and Adults (GIDYQ–AA), a 27-item scale originally developed by Deogracias et al. (2007). In Study 1, adolescents with GID (n1⁄444) were compared to CC adolescents (n1⁄498); and in Study 2, adults with GID (n1⁄441) were compared to CC adults (n1⁄494). In both studies, clients with GID self-reported significantly more gender dysphoria than did the CCs, with excellent sensitivity and specificity rates. In both studies, degree of self-reported gender dysphoria was significantly correlated with recall of cross-gender behavior in childhood—a test of convergent validity. The research and clinical utility of the GIDYQ–AA is discussed, including directions for further research in distinct clinical populations.” (abstract, Singh 2010)
————
References
Deogracias JJ, Johnson LL, Meyer-Bahlburg HFL, et al. The Gender Identity/Gender Dysphoria Questionnaire for Adolescents and Adults. 2007. The Journal of Sex Research 44(4):370-79.
Singh D, Deogracias J, Johnson LL, et al. The Gender Identity/Gender Dysphoria Questionnaire for Adolescents and Adults: further validity evidence. 2010. The Journal of Sex Research 47(1): 49-58.

Drawing this self portrait was a fascinating experience.
Before I ever start a drawing, I spend a lot of time analyzing the face in the reference photo, observing the technical aspects of facial proportions and composition and contrast, and figuring out how to capture the emotion in their expression. It’s an intellectual and artistic analysis done from a detached, non-judgmental, keenly observant, and empathetic perspective. This process has completely changed the way I see my own face in the mirror. Now I see my face with so much more interest – what’s unique about her face? how would I capture her expression there? – now I see my face with so much more compassion.
Drawing my self portrait (titled #1 because I think there will be more!) was very strange at first, like an out-of-body experience, similar to my mirror experiments but more prolonged and more precise. I deliberately drew all the facial imperfections that have long been a source of self-consciousness for me: acne scars on my left cheek, the vein that so prominently traverses my left temple, right iris heterochromia.
After I finished the sketch, I realized that I actually like my eyes – they are very big, very expressive, and asymmetrically colourful. I also like my collarbones and the upper pectoral definition on my chest, the hard-earned result of thousands of pushups. And I’ve always loved my short, messy hair.
I never thought I would be capable of drawing my own face. My self portrait took six hours to complete… six hours staring at my face, after six years of showering in the dark and avoiding mirrors with pathological self-loathing.

Materials: ballpoint pen (black) + black fine-point Sharpie marker + Staedtler colored pencils
Time: 6 hours
Reference: photo of myself taken July 16, 2016 on the stairs at a city train station. I chose that photo because the lighting provided good contrast and the cautious, wary facial expression is characteristic of my chronic skepticism.
Comments: I sign most of my drawings as TM. But I have as many names as I do clothes, so when I started drawing again, I was initially unsure what my signature should be. Most commonly I go by Thomas or by my given name (which starts with J), so I decided to sign with a provisional TM. I can turn the T into a capital J with a single curved stroke of the pen if I want. I signed this self portrait with JM because my given name and the face I drew have been mine my whole life. Thomas is a newer addition.
Irene Adler: Do you know the big problem with a disguise, Mr. Holmes? However hard you try, it’s always a self-portrait.
Sherlock Holmes: You think I’m a vicar with a bleeding face?
Irene Adler: No, I think you’re damaged, delusional and believe in a higher power. In your case, it’s yourself. And somebody loves you.
– BBC Sherlock (S02, E01 – A Scandal in Belgravia)

I have been one acquainted with the night,
I have walked out in rain – and back in rain.
I have outwalked the furthest city light.I have looked down the saddest city lane.
I have passed by the watchman on his beat
And dropped my eyes, unwilling to explain.One luminary clock against the sky
Proclaimed the time was neither wrong nor right.
I have been one acquainted with the night.– Robert Frost
(Acquainted with the Night, 1928)
